Carpal Tunnel Syndrome: What We Know
Although CTS is a strong driver of workers' compensation costs, lost wages, lost productivity, and disability, there is still a limited understanding of its frequency and causes in working populations.
- By Blake McGowan
- Jun 01, 2018
Carpal tunnel syndrome (CTS) is one of the most common work-related musculoskeletal disorders (MSDs) and is a widely recognized condition. Chances are, you probably know someone who suffers from it, had surgery to alleviate the painful symptoms of it, or has it but doesn't know it yet. Even though the incidence is so great and could be one of the most talked about ailments at dinner parties, most people might not know or understand its etiology.
What is Carpal Tunnel Syndrome?
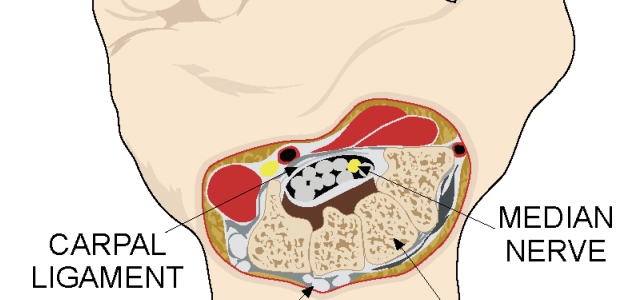
To fully understand the disorder, it's important to know how the arm works. Tendons, blood vessels, and the median nerve pass through the carpal tunnel (at the wrist) as they make their way from the forearm to the fingers. The median nerve plays a significant role in how the hand functions. It controls the small muscles (which control movement) at the base of the thumb and enables the palm side of the thumb, index, middle, and part of the ring finger to feel sensations or touch. If the tendons and tendon sheaths running through the carpal tunnel become irritated and begin to swell, the median nerve may be affected, and carpal tunnel syndrome may result.
What Are the Symptoms?
Some people may not know they're at risk or that they have CTS because the symptoms are so gradual. Tingling, frequent burning, itching, and numbness are some of the early reported signs and generally appear in one or both hands during the night. In fact, most people sleep with flexed wrists, and those who suffer might try to "shake out" the "pins and needles" sensation. We all know what our foot or leg feels like when it is "asleep" or feels swollen from sitting in a pretzel-like position on the floor. Imagine feeling that often.
As the condition worsens, the sufferer may report more tingling, reduced grip strength, and the inability to grasp an object or perform certain tasks during the day. He or she may say his or her fingers feel useless. As the condition progresses, the muscle at the base of the thumb wastes away and the ability to distinguish hot from cold objects diminishes.
What is the Prevalence of CTS?
The prevalence of medically diagnosed and electrodiagnostic confirmed CTS is generally higher in the working population compared to the general population. The prevalence of CTS among manufacturing and meatpacking workers ranges from 5 to 21 percent. The prevalence in general populations ranges from 1 to 5 percent (Bonfiglioli et al., 2013; Dale et al., 2013; Fan et al., 2015; Harris-Adamson et al., 2015; Harris-Adamson et al., 2016; Kozak, et al., 2015; Violante, et al., 2016). The highest prevalence in the working population is among grinders, butchers, grocery store workers, frozen-food factory workers, platers, and other workers whose jobs involve high-force, highly repetitive manual movements. Jobs with the highest CTS risk include those in meat and fish processing industries, forestry work with chain saws, and electronic assembly work (Hagberg et al., 1992).
Incidence rates of CTS calculated from the Washington state workers' compensation records ranged from 0.8 to 14.8 per 1,000 person-years and varied by industrial and occupational classifications. Similar rates of 12.4 per 1,000 person-years were observed among 432 industrial and clerical workers using a case definition requiring electrodiagnostic confirmation. A pooled analysis of six prospective studies of 4,321 workers showed that:
- the prevalence of hand symptoms of CTS is 15.2 percent,
- the prevalence of CTS based on electrodiagnostic method is 7.8 percent,
- the incidence of CTS is 5.8 percent, and
- the incidence rate of CTS is 2.3 per 100 person-years.
What is the Cost and Burden of CTS?
CTS is the most expensive upper-extremity MSD. Medical care cost estimates in the United States exceed $2 billion annually and are primarily due to carpal tunnel release surgery. The non-medical costs are estimated to be 1 to 4 times greater than the medical costs (Dale et al., 2013).
In the United States, the median lost work time resulting from work-related CTS is 27 days. This is longer than that of any other work-related disorder, except fractures. Furthermore, 18 percent of workers who develop CTS reported leaving their jobs within 18 months (Dale et al., 2013).
Although CTS is a strong driver of workers' compensation costs, lost wages, lost productivity, and disability, there is still a limited understanding of its frequency and causes in working populations.
What are the Individual and Occupational Risk Factors?
There are both individual and occupational risk factors associated with CTS (Bonfiglioli et al., 2013; Dale et al., 2013; Fan et al., 2015; Harris-Adamson et al., 2015; Harris-Adamson et al., 2016; Kozak, et al., 2015; Violante, et al., 2016). Individual risk factors include age, gender, body mass index (BMI), pregnancy, medical conditions (e.g., diabetes and thyroid disorders), and musculoskeletal comorbidities (e.g., trigger finger, rotator cuff syndrome, cervical radiculopathy). Thus, aging, weight/obesity, gender (female), and existing medical conditions increase the risk of CTS.
A tremendous amount of effort and research has been conducted to better understand occupational risk factors for CTS. Many risk factors have been studied, including computer use, awkward postures, forceful exertion, repetition, vibration, and various combinations of these factors. However, the risk factors most strongly associated with CTS include the following:
- Time-weighted average peak hand force
- Forceful hand exertion repetition rate
- Percent time of forceful hand exertion
- Hand-arm vibration
Can CTS Be Effectively Managed?
There are many approaches to managing CTS following diagnosis. Most are considered conservative approaches, and their effectiveness varies greatly. Wrist splinting (holding the wrist in a neutral position during sleep) has been shown to be ineffective. Non-steroidal anti-inflammatory drugs (NSAIDs) have shown no evidence of effectiveness. Oral corticosteroids can be effective over short durations (two to four weeks), but they are highly toxic to the body and associated with several side effects. Local corticosteroid injections can provide short-term improvement in symptoms, but they tend to lose effectiveness after one month, and ultrasounds have revealed mixed results (Newington et al., 2015).
The most effective treatment following diagnosis is carpal tunnel release surgery. This surgery cuts the transverse carpal ligament, which releases pressure on the median nerve and relieves CTS symptoms. It has a success rate between 50 and 75 percent at reducing symptoms. However, the recovery time can be up to three months (Newington et al., 2015).
What's the Best Way to Manage Occupational Risk Factors for CTS?
The most effective way to reduce or manage CTS in the workplace is to design the workplace and work tasks to be within worker capabilities. This means providing engineering controls to reduce worker exposure to the known risk factors of force, repetition, duration, and vibration. This approach starts with completing a quantitative MSD risk assessment of the job to determine which tasks involve risk and what the magnitude of that risk is.
The American Conference of Government Industrial Hygienists (ACGIH) hand activity level (HAL) is an excellent risk assessment tool to assess hand, wrist, and forearm biomechanical overload based on exertions, frequency, and force use. The ACGIH threshold limit value (TLV) method can be used to predict CTS. A study of 4,097 workers found a dose-response relationship between the ACGIH HAL TLV classification and risk for CTS; higher risk scores are linked to higher rates of CTS (Bonfiglioli et al., 2013).
Once the magnitude of MSD risk is determined, the next step is to identify the root cause(s) of the risk. Controls are identified, prioritized, and then implemented to address the root cause(s). Effective controls either eliminate exposure or reduce the level of exposure to the risk factors. Controls that reduce time of exposure or rely on the worker to change behavior are less effective.
What's the Bottom Line?
CTS is one of the most common work-related MSDs and the most expensive upper-extremity MSD. There are few effective methods to manage it following diagnosis, other than carpal tunnel release surgery. In the workplace, the most effective way to reduce CTS is to proactively determine the magnitude of the risk and then implement engineering controls to reduce exposure to forceful exertions.
References
1. Bonfiglioli R, Mattioli S, Armstrong TJ, Graziosi F, Marinelli F, Farioli A, Violante FS. (2013). Validation of the ACGIH TLV for hand activity level in the OCTOPUS cohort: a two-year longitudinal study of carpal tunnel syndrome. Scand J Work Environ Health. 2013 Mar 1;39(2):155-63.
2. Dale AM, Harris-Adamson C, Rempel D, Gerr F, Hegmann K, Silverstein B, Burt S, Garg A, Kapellusch J, Merlino L, Thiese MS, Eisen EA, Evanoff B. (2103). Prevalence and incidence of carpal tunnel syndrome in US working populations: pooled analysis of six prospective studies. Scand J Work Environ Health. 2013 Sep 1;39(5):495-505.
3. Fan ZJ, Harris-Adamson C, Gerr F, Eisen EA, Hegmann KT, Bao S, Silverstein B, Evanoff B, Dale AM, Thiese MS, Garg A, Kapellusch J, Burt S, Merlino L, Rempel D. (2015). Associations between workplace factors and carpal tunnel syndrome: A multi-site cross sectional study. Am J Ind Med. 2015 May;58(5):509-18.
4. Hagberg M, Morgenstern H, Kelsh M. (1992). Impact of occupations and job tasks on the prevalence of carpal tunnel syndrome. Scand J Work Environ Health. 1992 Dec;18(6):337-45.
5. Harris-Adamson C, Eisen EA, Kapellusch J, Garg A, Hegmann KT, Thiese MS, Dale AM, Evanoff B, Burt S, Bao S, Silverstein B, Merlino L, Gerr F, Rempel D. (2015). Biomechanical risk factors for carpal tunnel syndrome: a pooled study of 2474 workers. Occup Environ Med. 2015 Jan;72(1):33-41.
6. Harris-Adamson C, Eisen EA, Neophytou A, Kapellusch J, Garg A, Hegmann KT, Thiese MS, Dale AM, Evanoff B, Bao S, Silverstein B, Gerr F, Burt S, Rempel D. (2016). Biomechanical and psychosocial exposures are independent risk factors for carpal tunnel syndrome: assessment of confounding using causal diagrams. Occup Environ Med. 2016 Nov;73(11):727-734.
7. Kozak A, Schedlbauer G, Wirth T, Euler U, Westermann C, Nienhaus A. (2015). Association between work-related biomechanical risk factors and the occurrence of carpal tunnel syndrome: an overview of systematic reviews and a meta-analysis of current research. BMC Musculoskelet Disord. 2015 Sep 1;16:231.
8. Newington L, Harris EC, Walker-Bone K. (2015). Carpal tunnel syndrome and work. Best Pract Res Clin Rheumatol. 2015 Jun;29(3):440-53.
9. Violante FS, Farioli A, Graziosi F, Marinelli F, Curti S, Armstrong TJ, Mattioli S, Bonfiglioli R. (2016). Carpal tunnel syndrome and manual work: the OCTOPUS cohort, results of a ten-year longitudinal study. Scand J Work Environ Health. 2016 Jul 1;42(4):280-90.
This article originally appeared in the June 2018 issue of Occupational Health & Safety.